Through a combination of observations in people and experiments in mice, researchers funded in part by the NIH’s National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) have uncovered the molecular underpinnings of bone loss associated with a condition in which too much parathyroid hormone (PTH) is produced. The findings, which appeared in the journal Cell Metabolism, suggest that treating patients with existing drugs may help prevent bone loss, sidestepping the need for surgery.
The parathyroid glands, which are four tiny glands that lie behind the thyroid at the base of the neck, help maintain the correct levels of calcium in the body by secreting PTH. People with hyperparathyroidism secrete too much of the hormone, which leads to loss of calcium from the bones and health problems such as fragile bones, kidney stones, and digestive symptoms.
Primary hyperparathyroidism (PHPT) occurs when there is a problem such as enlargement of one or more of the parathyroid glands. It is typically treated with surgery, but the invasive procedure is not suitable for everyone. The condition usually occurs randomly, but in rare cases it is caused by an inherited gene mutation. It is more common in women than men and most often strikes between the ages of 50 and 60.
While scientists have long known that excess PTH causes bone loss, the exact mechanisms underlying the process have been unclear. In this study, researchers led by Roberto Pacifici, M.D., of Emory University, in collaboration with physicians from the University of Turin, Italy, focused on the role played by a type of immune cell called a Th17 cell. Th17 cells recognize invading pathogens and secrete signaling molecules that intensify the immune assault on the microbe.
Earlier work had implicated Th17 cells in bone degradation. For example, studies had shown that they contribute to bone loss that accompanies estrogen deficiency in mice. In addition, other research had linked high numbers of Th17 cells with inflammatory conditions like rheumatoid arthritis and Crohn’s disease, which are associated with bone loss.
To determine if Th17 cells are involved in bone degradation in people with PHPT, Dr. Pacifici and colleagues compared blood cells from 20 PHPT patients in Italy to those from healthy controls. They found that the gene for a signaling molecule called IL-17A, which is primarily produced by Th17 cells, was more active in PHPT patients’ blood cells. Following surgery to remove parathyroid gland tissue, the IL-17A gene activity levels in patients’ blood cells returned to normal. These findings suggested that IL-17A and Th17 cells may be involved in the condition.
To further investigate the roles played by Th17 cells and IL-17A in PHPT, the researchers studied mice that had been continuously infused with PTH for a period of two weeks, mimicking human PHPT conditions. Similar to what they observed in PHPT patients, IL-17A gene activity was elevated in the mice’s blood cells. They also saw more Th17 cells circulating in the blood of these mice compared to non-treated mice. These results suggested that continuous PTH treatment caused an excess of Th17 cells and increased IL-17A production.
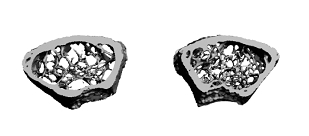
When they examined the bones of the PTH-treated mice, there was about a 25 percent decrease in bone density compared to controls. This harmful effect on the mice’s bones was prevented when they blocked IL-17A’s activity using an antibody. They also found that diltiazem, a drug used to treat high blood pressure, inhibited bone loss in the PTH-infused mice. Further experiments showed that diltiazem works by blunting PTH’s ability to stimulate Th17 cell multiplication and maturation.
These results implicate Th17 cells and IL-17A in PTH-induced bone loss, and suggest that targeting them may be an effective strategy for preserving bone mass in people with PHPT. Pending the outcome of future clinical trials, IL-17A antibodies and diltiazem could represent promising new treatment options.
"This work highlights the value of understanding the basic biology of a disease for improving clinical practice," said Dr. Pacifici. "Now that we know more about the mechanism of PTH-induced bone loss, we may eventually be able to avoid costly surgical procedures and instead treat patients with existing, widely used medicines."
This work was supported by the NIH’s NIAMS (grants R01-AR054625, K01-AR061453 and R01-AR059364), National Institute of Diabetes and Digestive and Kidney Diseases (grant T32-DK007298) National Center for Research Resources (grant S10-RR028009) and National Institute on Aging (grant R01-AG040013). The VA Office of Research and Development and the China Scholarship Council also contributed support.
# # #
IL-17A Is Increased in Humans with Primary Hyperparathyroidism and Mediates PTH-Induced Bone Loss in Mice. Li JY, D'Amelio P, Robinson J, Walker LD, Vaccaro C, Luo T, Tyagi AM, Yu M, Reott M, Sassi F, Buondonno I, Adams J, Weitzmann MN, Isaia GC, Pacifici R. Cell Metab. 2015 Nov 3; 22(5):799-810. doi: 10.1016/j.cmet.2015.09.012. Epub 2015 Oct 8. PMID: 26456334
The mission of the NIAMS, a part of the U.S. Department of Health and Human Services' National Institutes of Health, is to support research into the causes, treatment and prevention of arthritis and musculoskeletal and skin diseases; the training of basic and clinical scientists to carry out this research; and the dissemination of information on research progress in these diseases. For more information about the NIAMS, call the information clearinghouse at (301) 495-4484 or (877) 22-NIAMS (free call) or visit the NIAMS website at https://www.niams.nih.gov.